Organizing with NNU

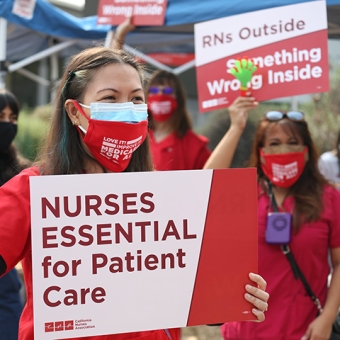
A union gives RNs the legal right to advocate as a collective for contracts that ensure safe working conditions, protect nurses’ rights, and improve wages and benefits so that we can focus on what we do best: caring for our patients. Read more »

Organizing: How it works
Every day more nurses organize to join the national nurses movement, meaning that we finally can speak with a unified voice. When RNs join together, it gives us protection for our patients and our profession.
Organizing: Know your rights
You have a legal right to organize under the National Labor Relations Act (NLRA), a federal labor law. In the case of many public hospitals, state law that is similar to the NLRA governs the process.

National Nurses United is the largest union of RNs in the United States, with a membership of more than 225,000 RNs in all 50 states. From coast to coast, we have won the best contracts for RNs in the nation.
Why RNs vote for NNU

New standards for RNs and patient protection
NNU contracts have created new standards for RN protection and include patient protection standards that give us the authority to directly improve patient care at our facilities.
Voice and respect
NNU representation provides RNs with the tools to have a real voice in patient care decisions, which we use to create safer health care facilities to protect our patients, our licenses, and ourselves.
A legally-binding contract
Your first NNU contract negotiations will provide you with an opportunity to work with your nurse colleagues to improve conditions for nurses and enhance protections for patients. With an NNU contract, your employer cannot unilaterally change your working conditions or reduce salaries and benefits.
Better salaries and benefits and a secure retirement
NNU nurses have won collective bargaining agreements that are the model for RNs across the nation and have won landmark improvements in retirement security for tens of thousands of RNs.
Videos
We can win anywhere; Nola nurses know
Here from nurses at University Medical Center in New Orleans, Louisiana on why and how they voted to join NNOC/NNU.
We can organize anywhere
Hear from nurses in Maine, North Carolina, and North Dakota on how and why they organized their hospitals.

Organize with National Nurses United to improve workplace standards through collective bargaining, reform national health care legislation, and make a difference for you and your patients.
Organizing victories



RNs at Orange County Global Medical Center vote overwhelmingly to join California Nurses Association
Bargaining victories



